
Breast Revision Surgery
There are various reasons why a woman would choose to undergo BREAST IMPLANT REVISION SURGERY. Some of the most common in Dr. Franco-Webb’s practice include a deflated saline breast implant, a desire to replace saline breast implants with silicone cohesive gel breast implants, correction of laterally displaced implants (with a wide central gap and no cleavage) or for inferiorly displaced implants (bottoming out).
Other reasons include capsular contracture (scarring of the tissue around the implants), droopy breasts, uneven breasts, ruptured gel implants, and the desire to change implant size, either smaller or larger. Less common, but more challenging, requests include correction of a double bubble deformity or for symmastia.
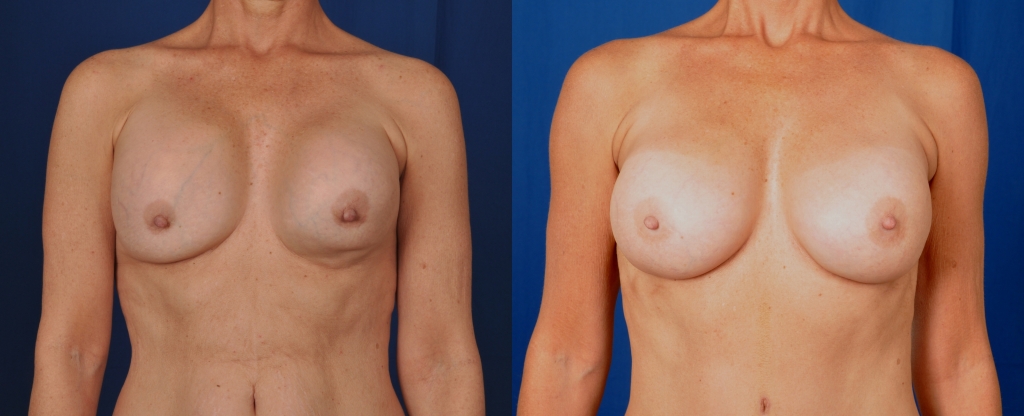
Deflated Saline Breast Implants
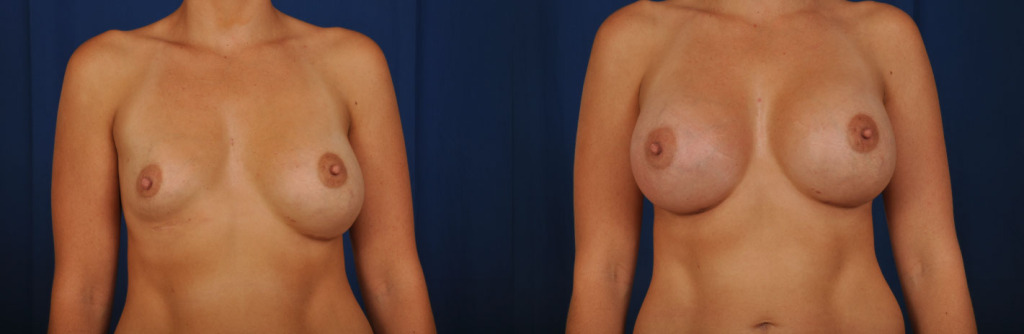
Before and after photos of a deflated right breast saline implant. Her saline implants were removed, her breast pockets were revised, correcting the creases, and cohesive silicone gel breast implants were placed.
Ongoing clinical studies attempt to accurately determine the average life expectancy of a breast implant. Due to so many variables, this research has been mostly inconclusive. However, based on previous studies, it is estimated that implants last approximately 10 to 25 years. Saline breast implants generally do not last as long as cohesive silicone gel implants.
Deflation of a saline breast implant can occur from a leaking valve or from a crack in the silicone elastomer bag. In Dr. Franco-Webb’s practice, the majority of deflated saline breast implants that she has removed have a leaking valve, demonstrating that the valve can become weak over time. The valve is the part of the implant that is used to fill the implant with saline at the time of the original surgery. Silicone cohesive gel breast implants do not have valves. Gel implants are pre-filled and sealed.
If a woman notices that her breast is getting smaller or is completely deflated, the saline (salt water) that is leaked out is absorbed by her body. She might feel the sensation of water running down the side of her breast. This deflation can occur slowly or it can occur, literally, over night.
Although a deflated saline breast implant does not require emergency surgery, a woman will usually want to have this corrected sooner rather than later. Also, it is recommended that surgery be performed optimally within a few weeks after deflation. This is because the capsule around the implant is collapsing and more internal surgery to re open the breast implant space, or breast pocket, will be needed the longer the waiting period.
If you have a deflated saline breast implant, Dr. Franco-Webb will make accommodations to see you within a day or two. It is very helpful if you bring in any information you may have regarding your implant manufacturer and size. This can be obtained with an implant device card that your original surgeon might have given you. Alternatively, medical records of your operative report can be obtained. Once you are seen by Dr. Franco-Webb, her staff will contact the manufacturer and start a case claim for you. Her staff will also obtain information regarding your warranty.
During your consultation with Dr. Franco-Webb, she will examine you and discuss your options which include removal and replacement of just the deflated implant. Other options include replacement of both implants with saline or with cohesive silicone gel. Sometimes a woman will take this opportunity to correct any breast pocket issues, to change sizes, or to undergo a breast lift along with the implant replacements.
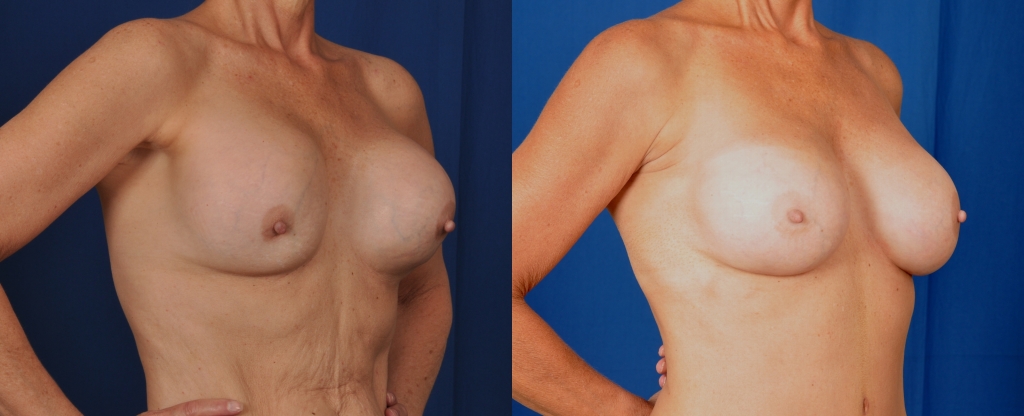
Desire To Replace Saline Breast Implants With Gel Breast Implants
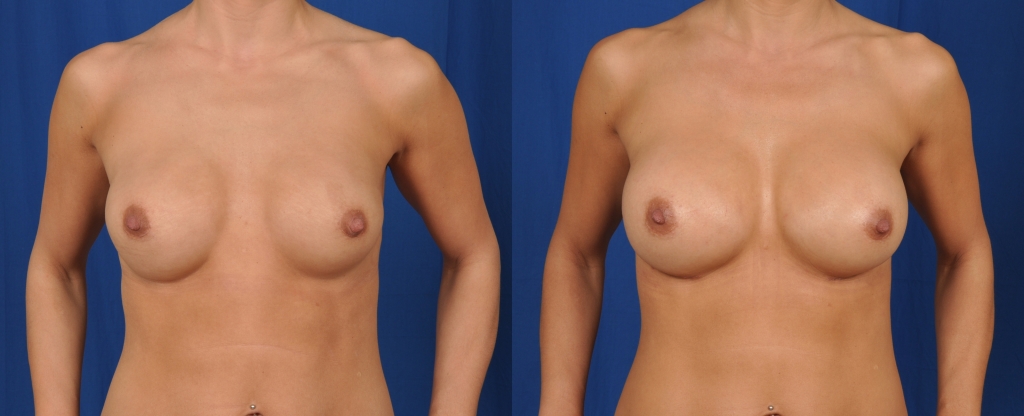
Before and after photos showing replacement of saline breast implants with gel breasts implants. Notice the correction of the superior breast rippling.
From the early 1990’s to November 2006 when the FDA re approved gel breast implants, women who desired breast augmentation surgery had only one option: saline breast implants. Since that re-approval in 2006, plastic surgeons have seen an increase in requests from replacing saline breast implants with gel breast implants. Some of the reasons for this request is to obtain a more natural feel and appearance with the gel implants. Also, saline implants have a higher incidence of rippling (wrinkling of the implant under the skin). Please go to the Breast Augmentation section to read more about cohesive gel implants, the consultation, the surgery process, and the recovery period.
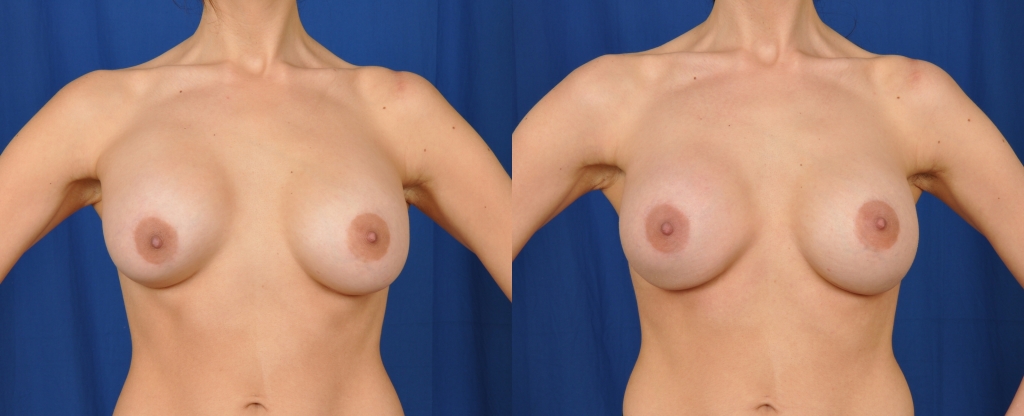
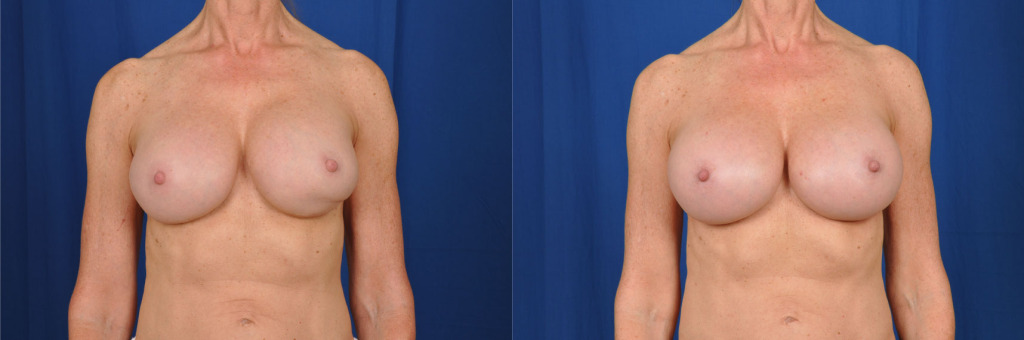
Displaced Implants, Laterally Or Inferiorly (Bottoming Out)

Before and after photos showing saline breast implant replacement with cohesive silicone gel breast implants and breast pocket revision for improved breast cleavage.
Implants can potentially become displaced over time, or might have been in a non favorable position since the time of the original surgery. Dr. Franco-Webb often sees patients who have had their surgery by another surgeon with these issues. She is able to correct these displacements by placing internal sutures (stitches) along the side of the breast, closing the space laterally so that the implants stay in an ideal position, achieving the patient’s desired amount of cleavage.
With inferiorly displaced breasts, or bottoming out, Dr. Franco-Webb is able to correct this also by placing internal sutures to raise the breast crease to the proper position. Please go to Breast Augmentation to read more about the consultation, the surgery process, and the recovery period.
Size Change

Before and after image of a patient who had her implants removed and replaced.
Women go through many changes during their lives. This includes pregnancy, breast feeding, weight changes and menopause. With these changes, their idea of the perfect breast size can also change. They find themselves wanting to increase or to decrease their breast implant size. When going down in size, a woman might also need a breast lift to re shape her breasts by removing excess skin and by repositioning her nipple placement. Please also see sections on Breast Augmentation and on Breast Lifts to read more about the consultation, the surgery process, and the recovery period.
Capsular Contracture
Before and after photos showing the results of a right breast pocket capsulotomy for the correction of a capsular contracture.
Before and after photos showing the results of a right breast pocket capsulotomy for the correction of a capsular contracture.
A capsule naturally forms around any foreign object placed within the human body. The body’s natural response is to wall off a foreign body, which includes a breast implant, whether silicone or saline. A capsule has been found to be formed from blood vessels, collagen and myofibroblasts. A capsule, optimally, should remain soft and pliable.
Capsular contracture is a potential risk following breast implant surgery. It may be more common following an inflammatory response involving an infection, hematoma, and seroma. The chance of it happening may increase over time. Capsular contracture occurs more commonly in patients undergoing revision surgery than in patients undergoing primary implantation surgery. Capsular contracture is a risk factor for implant rupture if the contracture because so severe that it causes the surrounding capsule to shrink and to cause pressure on the implant. It is one of the most common reasons for reoperation in augmentation and reconstruction patients. Symptoms of capsular contracture range from mild firmness and mild discomfort to severe pain, distorted shape of the implant, and palpability (ability to feel the implant).
Patients should also be advised that additional surgery may be needed in cases where pain and/or firmness are severe. This surgery ranges from removal of the implant capsule tissue to removal and possible replacement of the implant itself. This surgery may result in loss of breast tissue. Capsular contracture may happen again after these additional surgeries.
Capsular contractures can occur as soon as 4-6 weeks after the original surgery.
Capsular contractures can be identified from mild to very severe. The classic scale used by Board Certified Plastic Surgeons is the Baker Classification:
- Baker I capsule is a soft breast without significant scar tissue.
- Baker II capsular contracture is a palpable scar tissue around the bag; however, not visible.
- Baker III capsular contracture is associated with visible and palpable hardening, leading to a deformed shape to the breast.
- Baker IV capsular contracture, most severe, is associated with hardening, palpable, visible and often a cold, hard breast that is very painful to even mild palpation.
When a patient presents to our office with severe scar tissue, it is very important to determine the specifics as to the original surgery.
First of all, capsular contracture is significantly higher above the muscle than below the muscle. When breast implants are placed above the muscle or subglandular (retromammary), the rate is higher and it may be more difficult to fix these patients as the result of removing scar tissue with capsule may thin out the breast and lead to increased palpability and visibility of the bag.
Therefore, a breast augmentation that is performed it its original phase should be done subpectoral (behind the muscle), to allow for more coverage with the expectation that the patient will probably undergo a secondary surgery in the future. In other words, we almost always place our implants behind the muscle or using the dual plane technique (two-thirds under, one-third over laterally) in order to allow for this need for better muscle coverage, a more natural appearance and better results when breast revision surgery will be required. Surgeries to be performed with capsular contracture include capsulotomies and capsulectomies with or without implant exchange.
Capsulotomy
A capsulotomy is a procedure where the capsule is simply open and released with an electrocautery device. This allows for an expansion, more room and more volume space to the implant to occupy, to allow for a softer breast. “Otomy” in Latin means to release the scar tissue; however, not to remove it. This is often used for patients who have very thin amounts of breast tissue and if you were to remove the capsule they may have tremendous visibility, palpability and a very deformed appearance to the breast.
Capsulectomy
A capsulectomy should be performed when there is a thick amount of silicone and/or scar tissue around the implant and there is good coverage even after exenteration of the scar tissue to prevent visibility and rippling of the bag. Removing the capsule also may reduce the incidence of recurrent scar tissue, but this has not always been found to be the case. Just because the capsule is removed, does not mean that they will not reoccur.
It is extremely important to judge each patient as an individual and just because one person, for example, your girlfriend has scar tissue removed, does not mean that in your case it will be the best option, depending upon your physical anatomy of your breast and your chest wall, as well as the placement of your implants by your previous surgeon.
Remove Or Replace Breast Implants
Whether to remove or replace the implants depends upon your previous surgery. If the implants are in good shape and the implants are not ruptured, they often may be left in place and a new implant may not be required.
However, some studies have found that capsular contracture may be associated with micro infections and thereby removing the implants, replacing them with new ones after cleaning and irrigating the pocket with antibiotic solution, may help to reduce recurrent infection.
Most of the time, with a longstanding capsular contracture and implants that have been placed for several years, we like to replace the implants at the same time with new implants, silicone and/or saline.
Capsular contracture is one of the most common causes of women to have breast revision surgery. It can occur anytime after the surgery has been performed, from four weeks on.
Ruptured Gel Breast Implants
Before and after photos showing the results of replacement of ruptured old silicone gel implants, capsulectomies and replacement with cohesive silicone gel breast implants.
Before and after photos showing the results of replacement of ruptured old silicone gel implants, capsulectomies and replacement with cohesive silicone gel breast implants.
A ruptured gel breast implant can sometimes be detected by an abnormal breast shape, as in the photos above. Other ways of detecting a ruptured gel implant are by high resolution ultra sound, mammogram or MRI.
If a patient has a ruptured gel breast implant, the implant along with it’s gel contents are removed. The surrounding scar tissue, or capsule, is usually removed as was done in the above patient. At the time of removing a ruptured gel implant, Dr. Franco-Webb “power washes” the breast pocket and uses a solvent to soak up the residual gel. The patient above had gel implants that were over 20 years old. Those implants are gooey when removed. The newer cohesive silicone gel breast implants are easily removed as the cohesive gel sticks together, even with a break in the outer bag.
Double Bubble Deformity
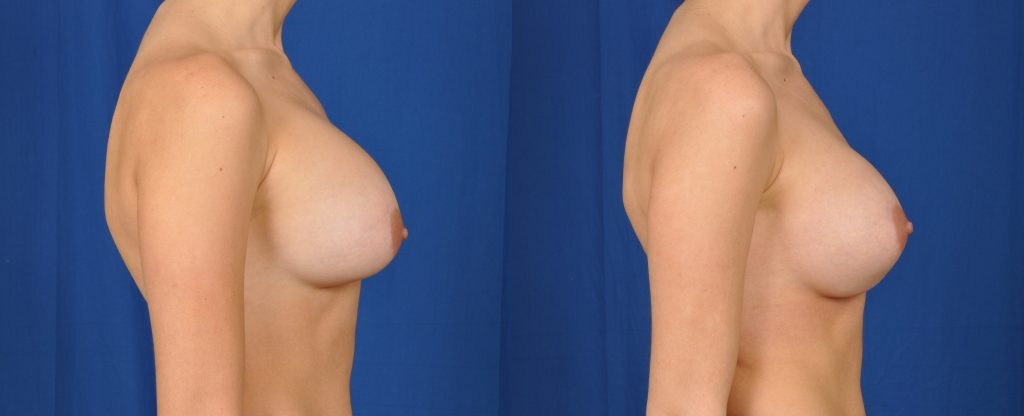
Before and after photo of a breast revision procedure.
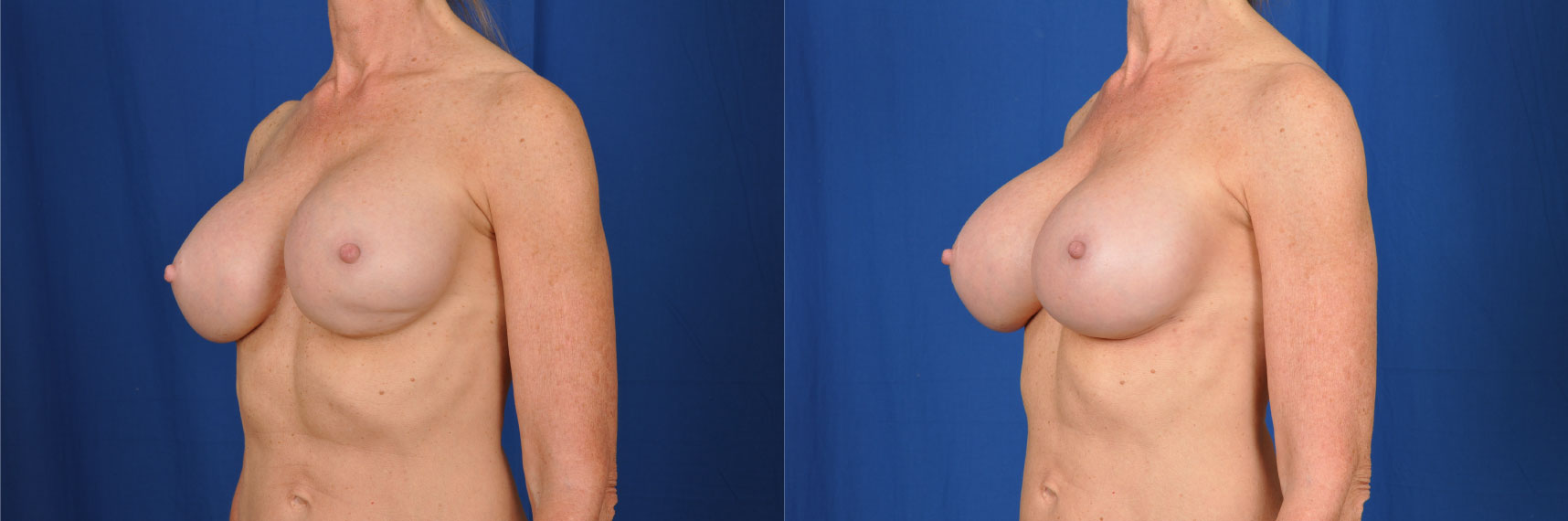
Before and after photo of a breast revision procedure (side view).
A double bubble deformity describes two round shapes on one breast, always located on the inferior breast in these case and as seen in the patient above. It occurs when an implant is placed below the original breast crease, which is done to accommodate an implant’s diameter so that it’s center is the nipple.
To correct a double bubble deformity, the glandular breast tissue is released with a cautery to allow for the breast tissue to lie smoothly over the implant, as was accomplished with the above patient. If the implant has dropped inferiorly to an abnormal position, the breast crease will need to be corrected with internal sutures (stitches) in order to correct the deformity.
Symmastia
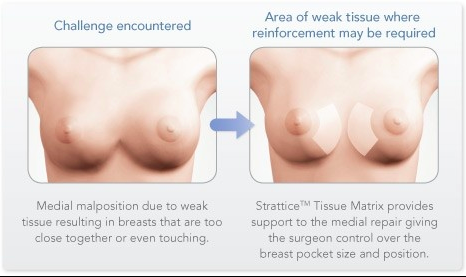
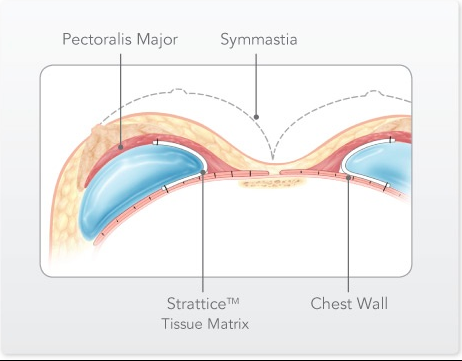
Symmastia is one of the most difficult problems to correct. It occurs when the implant crosses over the midline of the chest. For the more severe symmastia deformities, Strattice, or another dermal matrix inlay grafting material, is used as shown above. Also, a narrower and smaller implant is placed in order to prevent crossover of the implant. In less severe cases, sutures (stitches) are placed, tacking the midline under surface of the skin down to the sternum (breast bone) as well as using the patient’s own tissue (capsule) for reinforcement.